I have not gone gentle into disability. Each assistive concession, from buying my first cane to installing grab bars in the shower, was agreed to only after heated discussion, gnashing of teeth, and tears. Neal has cajoled me into the acceptance of things that make my life better at home, and we’ll talk more about them later. Today I’ll tell you about my journey from silent sufferer to squeaky wheel at work.
When I first walked up the white marble steps of the Folger Shakespeare Library, a beautiful, old, totally not handicapped-friendly building, I was an able-bodied 28-year-old. As the years went on, those stairs became more treacherous, especially when slick with rain. There was nothing to be done about them, though, so I either walked verrrrry slowly or entered through the rear of the building on wet or weak days.
Bathrooms were a different story. I worked in the basement where a men’s room with a single stall was between my office and the two stall women’s room. Having my bladder give up between these two pit stops occurred a few times before I finally wrote something akin to the following to the HR manager.
Hi there! Among the many gifts MS has bestowed upon me is a less than reliable bladder. Having to walk all the way to the ladies’ room is sometimes a hardship, and I wonder if maybe the men’s room could be converted to unisex. Thanks for your help.
Hi there! Among the many gifts MS has bestowed upon me is a less than reliable bladder. Having to walk all the way to the ladies’ room is sometimes a hardship, and I wonder if maybe the men’s room could be converted to unisex. Thanks for your help.
Shortly thereafter I got a reply saying that this was indeed a reasonable accommodation and that she would work on an announcement and ordering a new sign. Easy peasy.
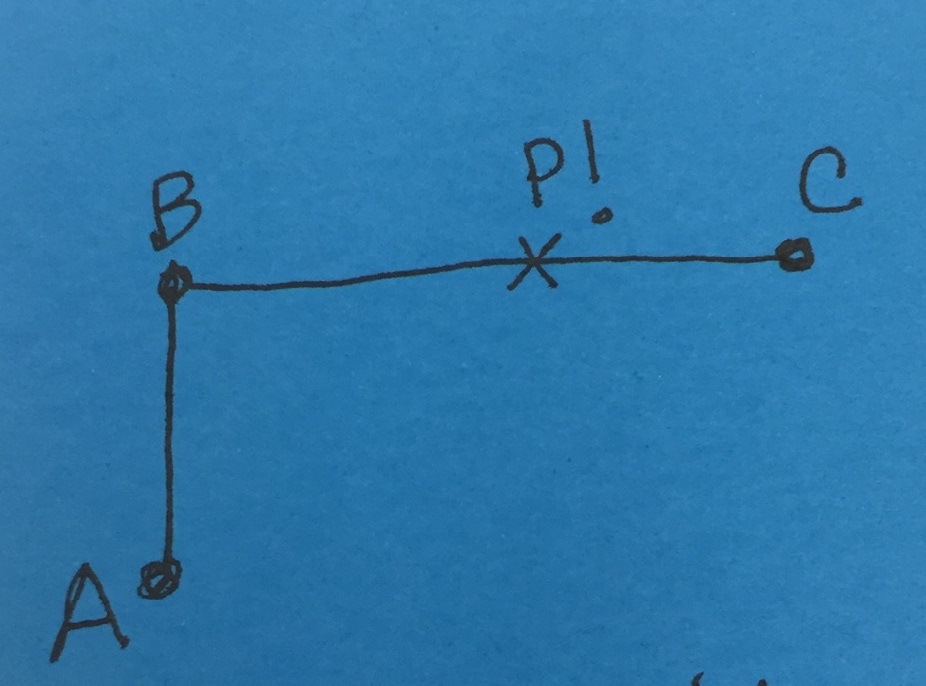 |
| A = office * B = men’s room * C = women’s room * P! = you get it |
When I moved to government work, I foolishly assumed that the office would be accessible. The government WROTE the Americans with Disabilities Act, after all! How could they not be friendly to the plight of the less mobile?
In so very many ways.
I won’t go into the challenges of entering either of the museum buildings from a wheeled device nor the shitty signage for the ramps and elevators that do exist. Not now, at least. I work in a modern office building with (hurrah!) a button operated door to enter from the sidewalk. The concierges are wonderfully helpful (see this post for proof) and take care of calling the elevator for me. Once on the correct floor, though, the problems began. The office could be entered by two sets of beautiful, ridiculously heavy glass doors. Heavy like, throw your entire body weight into pulling it open and then quickly wedge a shoulder against it so it doesn’t close while you recover from the strain of opening it heavy. Pushing through was easier but still a challenge. The break room doors were identical with the added bonus that one would usually pass through them with hot coffee or a week’s worth of snacks in one’s hands. Even strapping middle-aged (they don’t make ’em young here, y’all) men would see me throwing myself against these doors and say, “They are awfully heavy, aren’t they?”
Then there was the issue of the bathroom. In order to reach the women’s room I had to take 82 steps, pass through one set of the aforementioned glass doors, AND get my clumsy-ass hands to fit a key into a lock, turn that key, and then remove it. Come watch me do that on my best day when I have no pressing needs, and I assure you it will not be pretty. Doing it with a straining bladder (or worse)? Tragic.
So, barely a month into the new job, I talked to someone in HR about my concerns, and within two weeks an email went out about collecting everyone’s bathroom keys. The office was abuzz with excitement about that inconvenience being removed. I gave myself a tiny internal high five for making everyone’s lives better. One issue down, one to go.
A month and a half passed, and in November I was told that the glass doors would be adjusted so they required no more than five pounds of force to open (the ADA standard for interior doors).
Shortly after Christmas, I inquired about the status and was told we were “waiting on a part.”
In early March, the pantry doors were adjusted at last. There were some growing pains — near injuries thanks to people pushing/pulling too hard, which was a little hilarious to be honest — but, again, people were pleased.
In late April, still awaiting action on the entry doors, I reached out to the EEO coordinator to check in, saying, “I’m not the only disabled person on the floor presently – we have someone with a walking stick, someone on crutches, and two folks with slings.”
On May 19, almost eight months to the day from my initial email to the HR manager, the entry doors were adjusted. And there was much rejoicing. On my part, at least.
I realize this hasn’t been the most engaging post, but there is an important message. If you need help, advocate for yourself. If you’re lucky enough to have an EEO office, start there; if not, HR should be a good bet. If you’re among those not yet needy, keep your eye out for how your workplace (or any place) might be unfriendly to gimps like me and speak up if you think adjustments should be made.
Squeak your ass off until necessary change finally happens.